

Unidos contra la Covid-19 @La_resistensia_@qoto.org
Divulgación de medidas contra la Covid-19. Actualidad científica.
Joined Dec 2022
❗Muy arriesgada la afirmación de Christian Drosten: "En mi opinión, la pandemia ha terminado."🤔
Y más viendo cómo China sufre la mayor ola de #Covid_19 desde el inicio de la pandemia.
Ojalá acierte 🙏
Christian Drosten zur Corona-Lage in Deutschland: „Nach meiner Einschätzung ist die Pandemie vorbei“
https://www.tagesspiegel.de/wissen/corona-experte-drosten-nach-meiner-einschatzung-ist-die-pandemie-vorbei-9089959.html
@Billius27@mstdn.ca in Spain too
Unidos contra la Covid-19
boosted

My spreadsheet of #COVID19 studies showing longer-term damage to the body has grown to 100 studies. Here's a link and a thread of some of the most interesting. The conclusion is that COVID can attack many parts of the body, remain present in the body, increase risks of serious cardiovascular, brain, lung and immune system disorders, and increase risk of death and disability. Stop taking it so lightly!
https://docs.google.com/spreadsheets/d/12VbMkvqUF9eSggJsdsFEjKs5x0ABxQJi5tvfzJIDd3U/edit?usp=sharing
@mcvmaaay97@mastodon.social Merry Christmas to all who celebrate. May your holiday be joyful, peaceful, and safe. #MerryChristmas2022 #JoinIn https://mastodon.world/@demsoc1973/109575419256374271
@mcvmaaay97@mastodon.social Con juventud no se debe decaer. Nunca🤗
@mcvmaaay97@mastodon.social ✌️💪
Children aged 10 to 19y played the greatest relative role in propagating Omicron epidemics, particularly when schools were open, followed by children aged 0 to 9y and adults aged 20 to 29y, as well as adults aged 30 to 49y. Persons aged over 50y played a more limited role in propagating Omicron infection in the community. #COVID19
https://www.medrxiv.org/content/10.1101/2022.12.22.22283867v1
Unidos contra la Covid-19
boosted

RT @TRyanGregory@twitter.com
Huh. So kids do transmit COVID, just like every other respiratory virus. 🤷♂️
https://www.medrxiv.org/content/10.1101/2022.12.22.22283867v1
🐦🔗: https://twitter.com/TRyanGregory/status/1606633335450750976
@mcvmaaay97@mastodon.social Sin datos parece que no hay pandemia, pero nada cambia y el virus sigue a lo suyo.
COVID spreads rapidly in China in what could be the worst surge of the pandemic. #COVID19
https://www.wbur.org/hereandnow/2022/12/23/china-covid-surge
Unidos contra la Covid-19
boosted

COVID minimizers and deniers have been wrong every step of the way:
- Mass infection didn't give us herd immunity, it left millions dead/disabled globally
- Masks and stay-at-home orders reduced spread
- Schools were transmission hubs
- Kids have died/gotten long COVID
- Vaccines have saved millions
But being wrong hasn't stopped them from publicly fantasizing about holding public trials/executions of public health officials.
Qingdao enfrenta medio millón de contagios diarios de COVID
La urbe china de 10 millones de habitantes enfrenta "un período de rápida transmisión y se acerca a un pico", advierten las autoridades. #COVID19
https://www.dw.com/es/qingdao-enfrenta-medio-mill%C3%B3n-de-contagios-diarios-de-covid/a-64203652
@mcvmaaay97@mastodon.social Feliz Navidad ❣️🤗
Feliz Navidad🎄y venturoso año nuevo 2023.☃️
Merry Christmas🎄 and happy new year 2023.☃️
Unidos contra la Covid-19
boosted

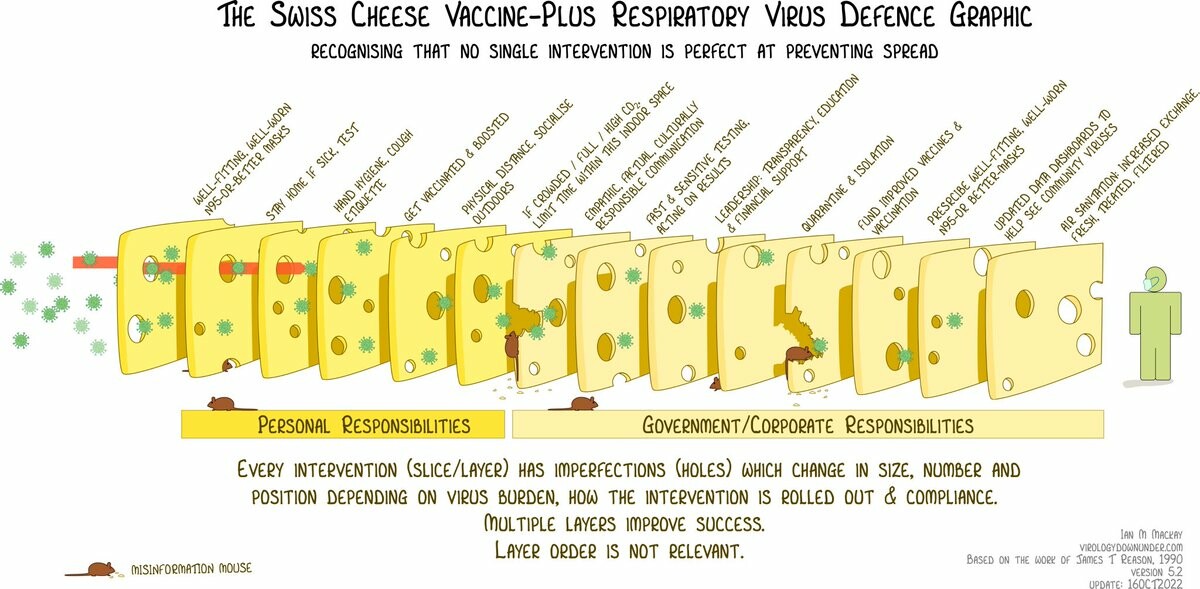
RT @LiangRhea
It's awful seeing China become a natural experiment for what happens when a country with a well developed health system and a highly masked popn lifts #COVID19 controls without sufficient vaccination. It's Swiss cheese- we should learn. ALL mitigations are required.
HT @MackayIM
248 million in China infected. #COVID19
https://youtu.be/3tdRb5coxJE
A Shanghai hospital has told its staff to prepare for a "tragic battle" with COVID-19 as it expects half of the city's 25 million people will get infected by the end of next week.
https://news.sky.com/story/covid-in-china-half-of-shanghais-population-of-25-million-could-be-infected-by-end-of-next-week-12773063

{kind=link}
{kind=link}
{kind=link}
Divulgación de medidas contra la Covid-19. Actualidad científica.
Joined Dec 2022
