

nikomer75 @nikomer75@qoto.org
phD Engineer
Joined Nov 2022
nikomer75
boosted

Our paper opn #LongCovid #Stigma now pulihsed in PLOS ONE. Summary of findings here: https://theconversation.com/long-covid-stigma-may-encourage-people-to-hide-the-condition-194939
nikomer75
boosted

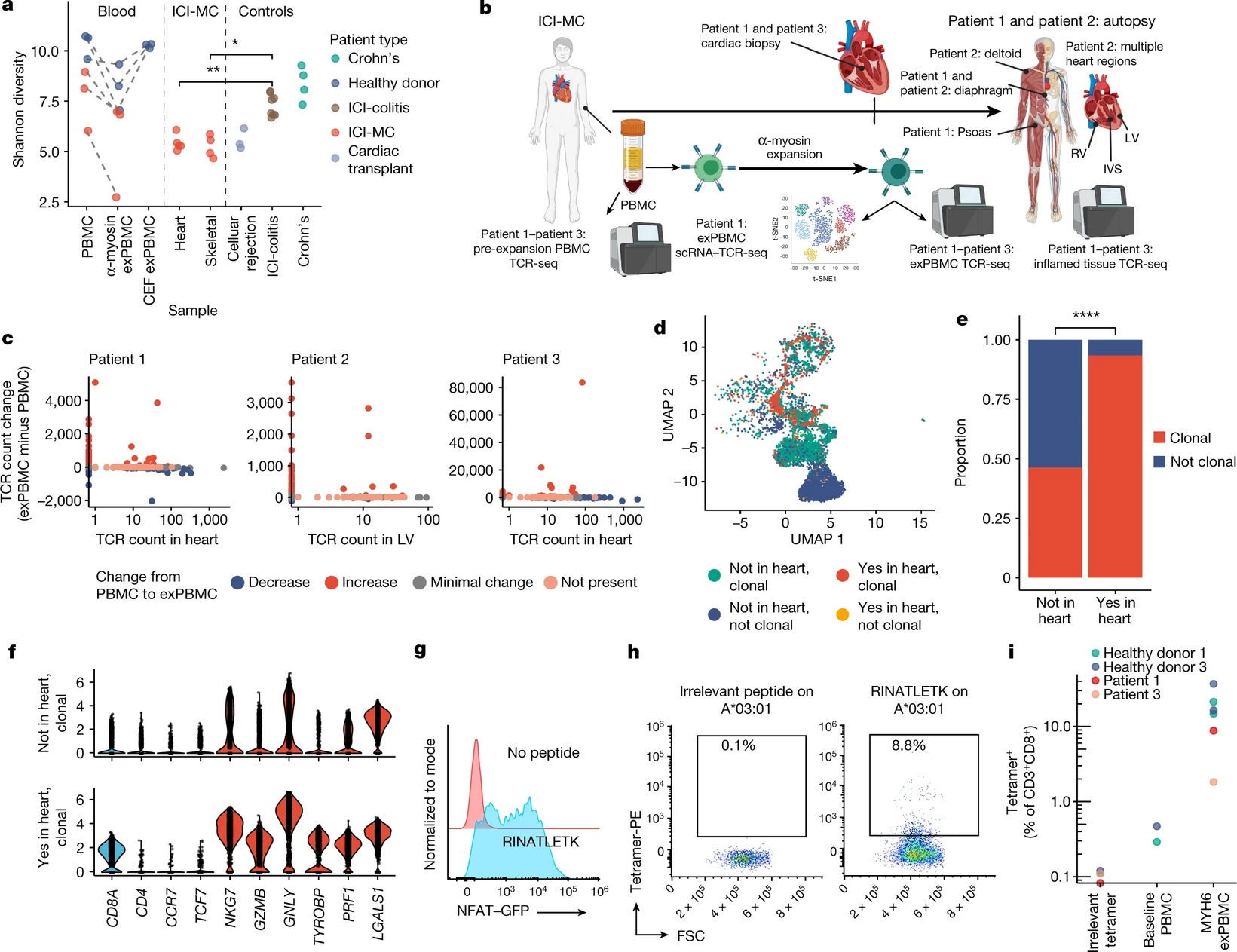
Here's a terrific new paper from one of my classmates about #ImmuneCheckpointInhibitor induced #myocarditis. This work finds that CD8+ T-cells are the critical mediator of heart inflammation, and identifies the alpha-myosin cardiac protein as a candidate autoantigen: https://www.nature.com/articles/s41586-022-05432-3 #science #medicine #immunology #cardiology #oncology #Tcell #genomics #scRNAseq
Tuberculosis, Like Covid, Spreads by Breathing, Scientists Report
https://www.nytimes.com/2021/10/19/health/tuberculosis-transmission-aerosols.html
Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin
https://cardiab.biomedcentral.com/articles/10.1186/s12933-021-01359-7
Liver injury in hospitalized patients with COVID-19: An International observational cohort study
https://www.medrxiv.org/content/10.1101/2022.11.06.22282006v1
Innate immune response to SARS-CoV-2 infection contributes to neuronal damage in human iPSC-derived peripheral neurons
Fatal COVID-19 outcomes are associated with an antibody response targeting epitopes shared with endemic coronaviruses
Aerosols from speaking can linger in the air for up to nine hours
“Is COVID-19 Dysregulating Our Immune Systems? "
https://twitter.com/MamaToronto/status/1594694013319356416?s=20&t=2jDrr72yLhtSIRlowLB9yg
ASYMPTOMATIC OR LATENT PERSISTENT INFECTION IN CHILDREN.
SARS COV-2 WAS DETECTED IN BIOPSIES OF TONSILS OR ADENOIDS
IN 25% OF ASYMPTOMATIC CHILDREN
None had experienced signs or symptoms
Authors point out:
lymphoid tissue may be a Reservoir of SARS-CoV-2
https://www.sciencedirect.com/science/article/pii/S1808869422001392?via%3Dihub

nikomer75
boosted

Sat down to eat at a "Saizeriya" (Japanese Italian chain) restaurant in Tokyo and immediately noticed the CO2 meter on top of the UV-C disinfection box on top of the counter. Wow.
I've seen the CO2 meter at several restaurants including a ramen place and an okonomiyaki restaurant, and now I'm seeing UV-C. Japan is so far ahead in recognizing #COVIDisAirborne. #COVID19
nikomer75
boosted
RT @ChrisCarrollMD@twitter.com
The longer this peds respiratory virus surge goes on, the more convinced I am that (similar to Measles) COVID has adversely affected children’s immunity in ways we don’t yet understand.
🐦🔗: https://twitter.com/ChrisCarrollMD/status/1594384723392225280
nikomer75
boosted

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Remember when leaders ended public health measures claiming that they could always reinstate them when hospitals were overwhelmed again? Well, that’s happening now. Where are the mask mandates? Where is the urgency?
https://www.washingtonpost.com/health/2022/11/20/hospital-capacity-rsv-flu-covid/
{kind=link}
phD Engineer
Joined Nov 2022
