
Reading about #SickDayRules and revisiting this very useful paper, thanks @LaurieTomlinson
#CJKHD
https://journals.sagepub.com/doi/abs/10.1186/s40697-015-0044-y

@cmclase @LaurieTomlinson on RASi - what I find fascinating is data from the COVID RAS studies, eg BRACE CORONA, REPLACE COVID @jordy_bc - and soon CLARITY
None of them show benefit of course, but it’s 🤯that continuing RASi in hospitalized COVID, or even starting RASi (CLARITY) didn’t cause harm.
We should really rethink sick day rules!
@hswapnil @LaurieTomlinson @jordy_bc
Yes and thank you for all those refs - will incorporate!
Thinking #SickDayRules for #CKD need a rethink!

@jordy_bc @cmclase @LaurieTomlinson since I am on a roll 😎
What about flozins?
Yes you can see euglycemic DKA in a small number, but
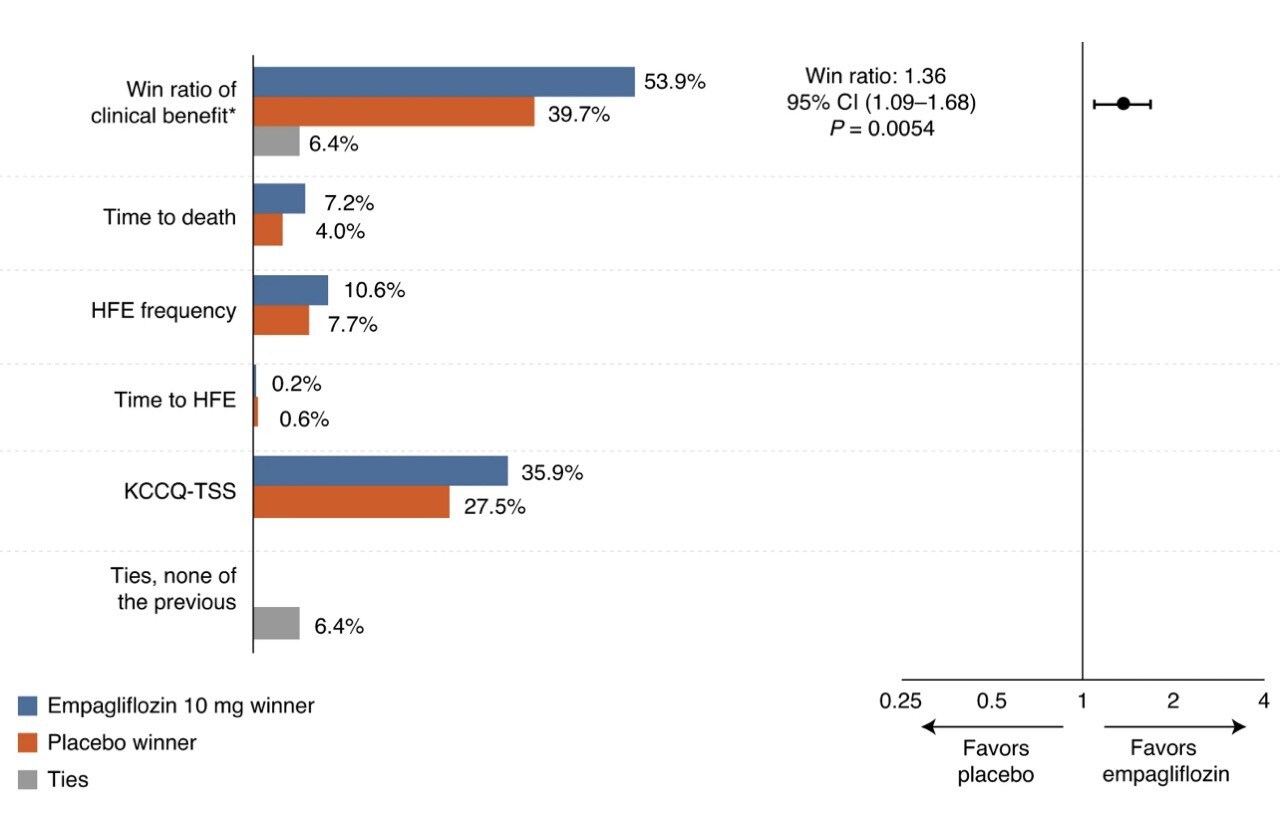
- EMPULSE shows benefit starting with acute decompensated HF https://www.nature.com/articles/s41591-021-01659-1
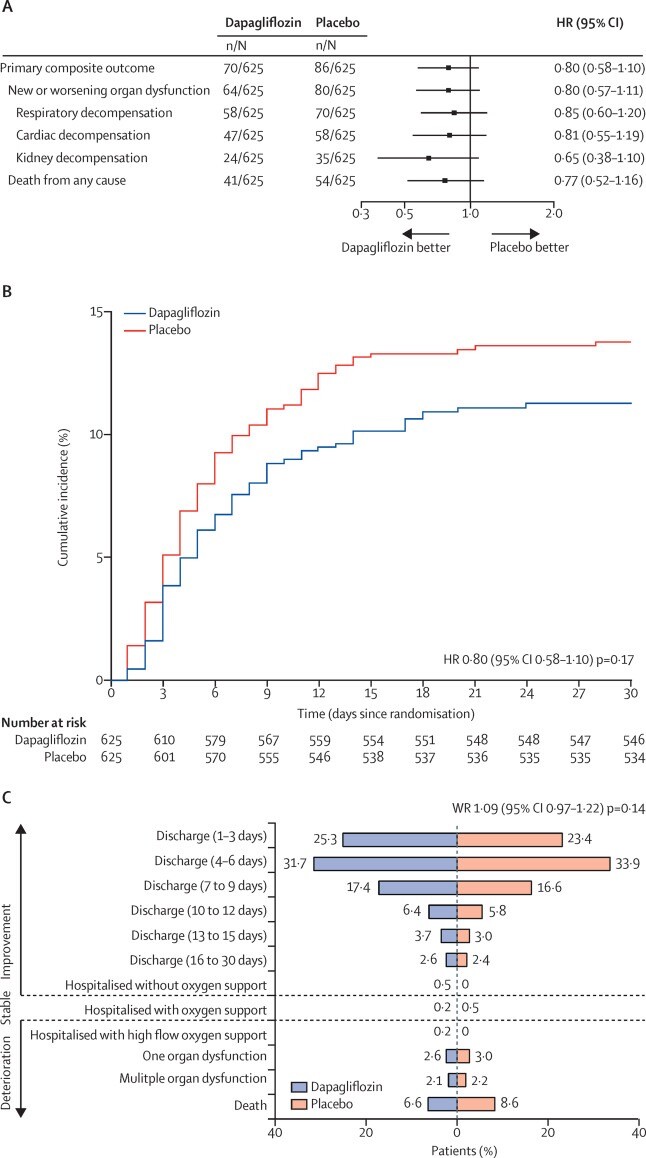
- DARE showed no harm starting DAPA in peeps hospitalized with COVID
It’s not stop flozins for all when sick - we need nuanced guidance🤔

{kind=link}
{kind=link}
@cmclase @LaurieTomlinson @jordy_bc @hswapnil This is the way. The question is not how early benefit accrues from SGLT2i (or RASi) but when it is safe to start. I’ m a critical care #flozinator😅
@load_dependent @LaurieTomlinson @jordy_bc @hswapnil
Maybe the rule is: stop #flozins when fasting. Any info on 12-18h fasts as in Ramadan or intermittent fasting?

More on #SickDayRules
And this one by @LaurieTomlinson herself
shows higher incidence rate ratio for gastroenteritis (IRR 43, compared with baseline) compared with LRTI and UTI s as risk of #AKI in new users of anti-hypertensives
No evidence of a difference in #AKI risk #RASi vs other agents for gastroenteritis or LRTI (interaction p >=0.78) weak evidence for UTI (interaction p=0.02; not robust in sensitivity analysis)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5796801/