
> is it? Here’s the study (linked below). It’s a meta-analysis from earlier in the pandemic, which looked at studies that included hospitalized and ambulatory patients.
Yes that is what the study is on. In other words.
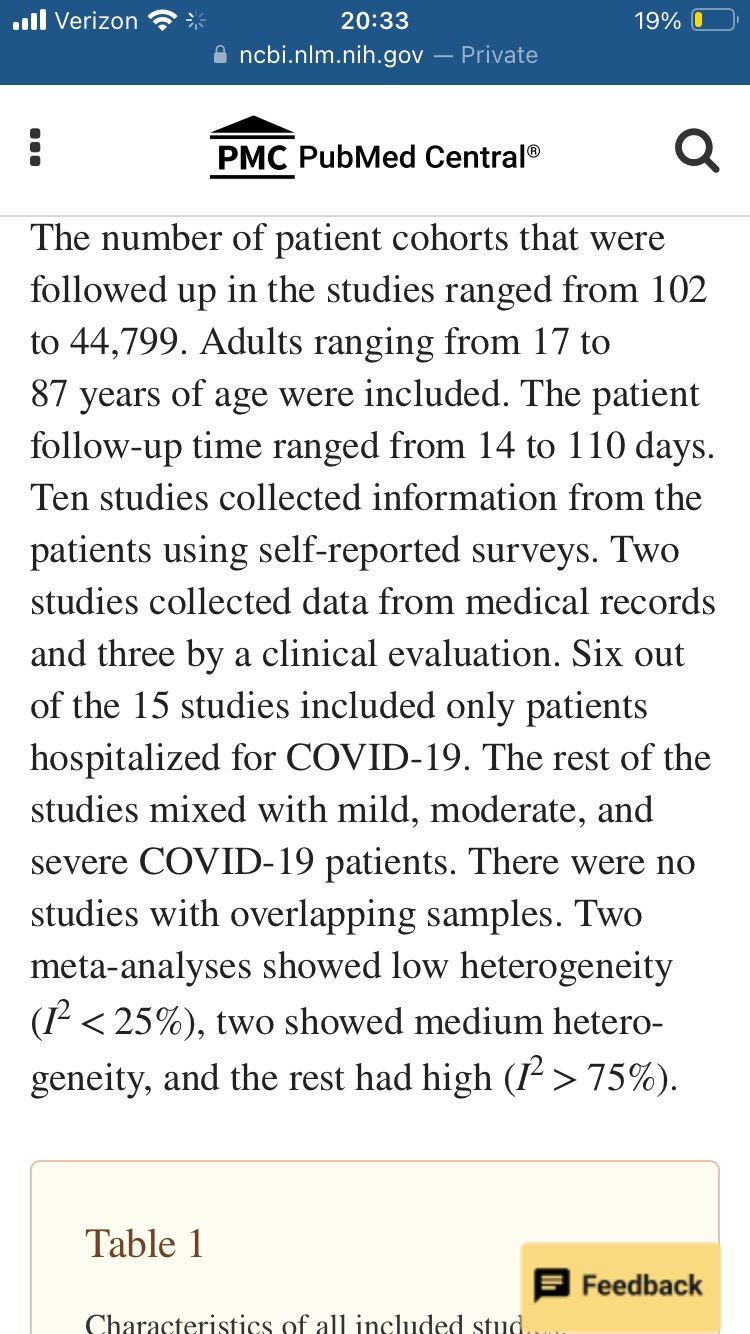
> The study concludes jn multiple places that 80% of people with COVID will experience one or more long-term symptoms.
No that is NOT what the study concluded. The Study concluded that Of people who have severe COVID, to the point of hospitalization, those people have an 80% chance of showing long term symptoms.
What it is NOT saying is that 80% of people who get COVID will have long term symptoms. These are two entierly different assertions.
You are trying to generealize a statement specifically made about hospitalized patients to apply to everyone who has ever had the disease. That is disinformation or negligence, im not sure which. You should have been taught better in school than to make that leap.
> Do I think that’s representative? No. Is it what the study says, yes.
Then you are wrong and it is negligence, that is very much **not** what the study says.

And did you read the part where they said that among studies that included all covid patients the range was up 10% to 35%.. they explicitly state the 80% was only limited to the hospitalized group.
So again, saying people with covid show up to 80% prevelance is disinformation.
I quoted this earlier do I need to go find it again?
Even the screen shotted quotes more or less agree with me if you read them carefully. The last screen shot for example talks about how quite a few of the studies in their meta analysis, nearly half, were limited to hospitalized patients. So no suprise that some of the studies in their metanalysis showed 80% figures.. again this is not intended by the study authors to be making the claim you seem to be saying it makes.
For what its worth I decided that you are probably operating in good faith at this point. I think you mean well. I also think its less about incompetance so much as crippling bias/agenda that may impede your competence. Understandable as you probably have seen the very real harm from the disease.

{kind=link}
@freemo @mcnado
As someone who was actually crippled by the disease, I do think that you underestimate how serious a situation things were in 2020, especially when you say there was overreaction and panic. There were people in the government literally arguing that we should allow the entire population to be infected so that we could move on as quickly as possible, while doctors were screaming at them that there was no evidence that people couldn't have repeated serious infections, and that we didn't know what the long-term consequences would be.
The people who wanted to let the entire population get infected called the doctors "alarmist".
We now have a dozen variants, 10 to 20% of people who got it have serious long-term consequences, and managed to develop a vaccine to prevents those consequences within months. If it had been taken more seriously until the vaccine was out, as the "alarmist" doctors wanted us to, we would not be where we are now.
> As someone who was actually crippled by the disease, I do think that you underestimate how serious a situation things were in 2020, especially when you say there was overreaction and panic.
I am sorry you've been crippled by the disease. :(
I didnt say it was overhyped at the start of the disease. Depending where in the timeline of the disease we are talking there were points where I would agree, particularly in the early days, it was at times under-hyped. It wasnt until it became political that the misinformation and over-hyping kicked in, which didnt come until later in the disease lifecycle.
More quarantine was not the answer, never was. But better hospital care and supporting care certainly would have saved lives. There is always room for improvement.
> There were people in the government literally arguing that we should allow the entire population to be infected so that we could move on as quickly as possible, while doctors were screaming at them that there was no evidence that people couldn't have repeated serious infections, and that we didn't know what the long-term consequences would be.
Actually I am one of the scientists that invented one of the algorithms that is fairly instrumental in this part of the discussion. I worked on a model for the DoD many years ago that models disease proliferation in populations. It can model the effect of vaccine, quarantine, and natural immunity.
To be clear, no doctors were not screaming for more quarantine, I was literaly one of those people part of the discussion (and fairly well known in the scientific community a a result). I can tell you as an authority as one of those Scientists, no we werent all screaming for more quarantine. In fact it was far more nuanced than that.
One prime example I can give to the nuance is your statement about variants. You seem to be under the false impression that quarantines would have resulted in fewer variants around today. The reality is quarantines can in fact increase the number of variants due to the conditions needed for new variants to become established in the population, which is assisted by small isolated groups of people more than large interconnected populations where there is no isolation.
It again comes down to the nuance of how new variants come into existence and become established, its not as simple as people think where it just happens spontaneously and then it exists. Variants usually require multiple mutations occurring in a series and need to become established so they must **locally** out compete the dominant strain and reach critical numbers before being released to the general population.
Keep in mind this is very different than other types of viruses, where recombination can occur in a single step.

@freemo @Raccoon Dude. You are not reading the same paper. You are so tied up on being right that you are confused. Again, READ the source I am citing which is NOT that Nature paper. Fuck…
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8352980/